Introduction — A lab morning that changed how I think about testing
I still remember a rainy Thursday in 2017 when a shipment of polymer-coated catheters arrived at our Chelsea, MA bench and nothing matched the paperwork. That moment pushed me to rework how I approach biological evaluation across device portfolios. In my work I blend bench experience with regulatory reading; biological evaluation often sits at the center of product questions, timelines, and late-stage surprises (yes, the paperwork can bite). I write from over 18 years in medical device testing and regulatory consulting, and I want to share the practical steps I use to reduce rework and clarify decisions for teams of engineers and regulatory leads.

Early in my career I accepted long test cycles as an unavoidable cost. Over time I learned to ask different questions: which tests give actionable risk data, and which create false confidence? These are questions I still ask on Monday mornings. The rest of this guide unpacks common breakdowns in toxicological workflows, shows where hidden pain points live, and points to practical fixes you can apply on the next project.
Deep dive: why standard toxicological risk assessment processes fail
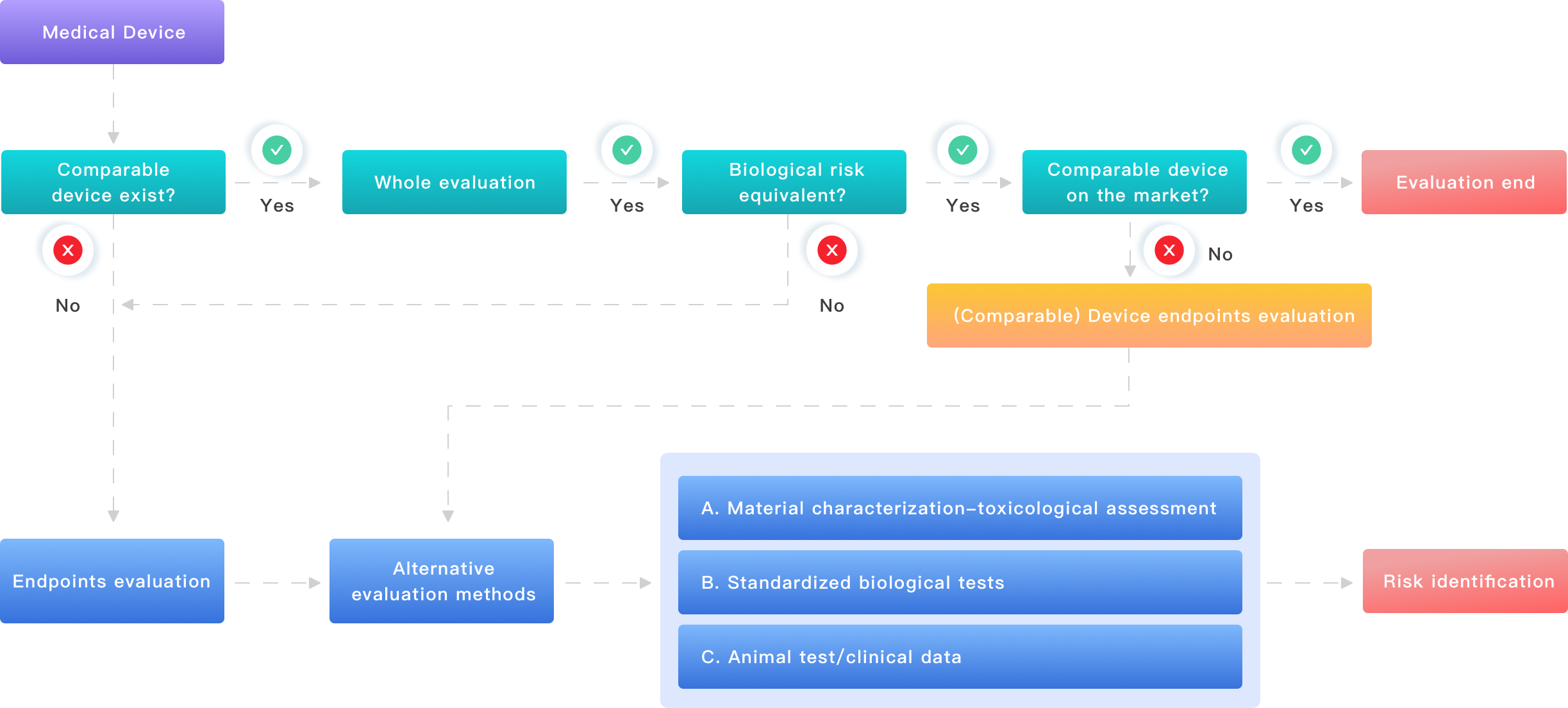
toxicological risk assessment is meant to translate chemistry and exposure into safety decisions. In practice, I see two recurring failures: poor assumptions about extractable/leachable chemistry and siloed communication between engineers, toxicologists, and test labs. These failures add weeks of delay. For example, on a 2019 cardiovascular stent project in Boston we spent ten weeks re-running extractables after an initial GC-MS screen missed a solvent residue; that oversight cost the program three review cycles and a late FDA hold. Those are the real costs, not the line items on an invoice.
What goes wrong?
First, teams often rely on blanket extraction conditions that do not reflect real-world exposure. I prefer designing extraction matrices around intended use (blood-contact vs. skin-contact) and to choose solvents and temperatures that mimic worst-case clinical exposure. Second, the Analytical Evaluation Threshold (AET) gets treated as a magic number. ISO 10993-17 helps calculate AET, but I have seen misuse where AET is applied without dose-response context. Third, lab reports focus on detection, not risk. A GC-MS hit list without hazard context—cytotoxicity assay results or dose-response—leaves toxicologists guessing. Look, I’ll admit—data without context frustrates me; it’s wasted effort.
Operationally, the usual fixes are slow: repeat testing, expanded chemistry panels, and over-conservative assumptions. Those add cost and, worse, they push product teams into defensive choices that can compromise design. On a surgical instrument program in 2021, an avoidable endotoxin retest inflated validation timelines by 30% because initial sterility sample points were mis-specified. The lesson: align test strategy to use profile and exposure early, not after data arrives.
Future outlook: integrating biological risk assessment into product lifecycles
Moving forward, I expect pragmatic blends of in-silico tools, targeted in vitro work, and smarter sampling to reduce cycles. A recent pilot I led (San Diego lab, Q1 2024) combined physiologically based pharmacokinetic modeling with targeted high-throughput screening. The team cut confirmatory assay time by roughly 40% while preserving confidence in decision-making. These are not theoretical gains; they come from matching method to question — and from early alignment between design engineers and toxicologists. The phrase “test everything” gives way to “test what changes risk.”
What’s Next — practical steps you can take
Start by building a short risk matrix for each new material or process change. Use three metrics when evaluating a new approach: (1) exposure relevance — does the test condition mirror clinical exposure? (2) decision value — will the data change what you do? (3) time-to-decision — how long until this result lets you move forward? In my consulting work I use those metrics to prioritize testing and to justify narrower, deeper analytical runs rather than broad, shallow screens. I also recommend a clear trace of sample origin — batch ID, sterilization cycle, and material lot (we tracked one PLA batch from June 2020 that explained a recurrent cytotoxicity spike).
To summarize: tighten your exposure assumptions, align labs to the decision question, and favor targeted analytics over broad fishing expeditions. I’ve used these steps on devices ranging from external fixation pins to implantable pumps, and they save weeks and reduce rework. For teams ready to scale this approach, consider external partners who provide integrated chemical analysis, toxicology consultation, and regulatory interpretation — they can plug into your project workflow and reduce coordination delays.
Three pragmatic evaluation metrics to help you choose a partner or workflow:
1) Time-to-decision under a known worst-case scenario (reporting days from sample receipt). I prefer partners who can give a fixed window. 2) Proven alignment to ISO 10993 series and documented AET calculations with underlying assumptions. 3) Evidence of casework: specific examples (device type, location, outcome). For instance, ask for a reference where a lab resolved an unexpected leachable in under six weeks and provided a rationale used in a regulatory submission.
I’m speaking from hands-on work spanning commercialization projects in the U.S. and EU, with clients ranging from small start-ups to mid-size OEMs. We learned the hard way that testing is not a checkbox; it’s a chain of decisions. If you want a pragmatic partner who focuses on decisions rather than just data, consider reaching out to Wuxi AppTec Medical device testing. I’ll keep iterating on these processes in the labs I work with—small steps, measurable gains, and clarity for the teams I advise.